#23 Resuscitative TEE with Dr. Ross Prager

On Critical Care Time we are - of course - HUGE fans of POCUS. On this episode, Nick and Cyrus take this love for POCUS to the next level with our discussion on Resuscitative Transesophageal Echocardiography (Resus-TEE) with Canadian intensivist, Dr. Ross Prager (@ross_prager) a Resus-TEE expert aficionado! On this show, we discuss the basics of Resus-TEE including indications, pitfalls and pearls, the practicality of implementing this modality at your hospital and some of the medico-legal considerations. We had a ton of fun recording his with Ross and hope you enjoy listening to it!
Quick Take Home Points:
Resuscitative TEE is a point of care ultrasound (POCUS) modality that allows rapid acquisition of high quality ultrasound images, even in patients where TTE imaging would be challenging.
Resus-TEE is particularly valuable in patients with undifferentiated shock, trauma, or cardiac arrest.
The risks of TEE are generally related to sedation & airway management. Critically ill patients who undergo resus-TEE are already intubated and sedated, thus these risks are minimized. There are risks of esophageal trauma with insertion, however these are probably comparable to the risks of gastric tube placement.
For operators who are already experienced at using POCUS, Resus-TEE skills can be acquired rapidly.
BONUS: Medicolegal liability with POCUS. More often liability is incurred by failure to perform POCUS when it is indicated than the converse. Overreliance on POCUS as a single datapoint is another potential source of liability.
Show Notes:
Written by Dr. Shane McMahon, DO
Edited by Dr. Nick Mark, MD
Hello Listeners! With these show notes we attempt to provide resources for those who prefer a written style of learning! All learning points are generated from discussions during each episode between expert guests and the CCT hosts with references added for additional guidance and learning opportunities. Thank you for listening and being a part of the Critical Care Time Community!
What is Resuscitative TEE?
Trans-Esophageal Echocardiography (TEE) uses a specialized ultrasound probe which is inserted through the mouth into the esophagus. This allows visualization of the heart from a posterior viewpoint, i.e. with the probe directly behind the Left Atrium.
This has several advantages over traditional trans-thoracic echocardiography (TTE) including:
Better windows even in challening situations (habitus, positioning, etc)
Better visualization during procedures (chest tube, CPR, etc)
Continuous visualization for serial assessments (e.g. repeat VTE measurements)
Analogous to POCUS, Resus-TEE is a goal directed TEE which aims to answer specific clinical questions as opposed to formal TEE which provides a global assessment of cardiovascular structure and function.

“Formal” vs “informal” ultrasound
Advantages of Resus-TEE?
What value does Resus-TEE add for the resuscitation and evaluation of critical patients when compared to traditional Point-of-Care Ultrasound (POCUS) Trans-Thoracic Ultrasound?
As with many imaging modalities there are 2 main steps to effective use: 1. Image acquisition and 2. Image interpretation.
With Resus-TEE acquisition can be made in seconds often with much better resolution compared to TTE. This is possible due to the nature of TEE, where factors like body habitus and technical skills can be bypassed directly into the esophagus.
Additionally because TTE probes can be left inside the esophagus for a extended duration (hours), enabling repeat imaging. This can be very useful for repeat measurements (e.g. LVOT VTI) to guide ongoing therapies.
Use Cases for Resus-TEE
Current core uses include:
Undifferentiated Shock (identifying etiology, determining response to resuscitation)
Cardiac Arrest (guiding CPR, identifying etiology)
Trauma
Procedural Guidance (specifically ensuring proper ECMO cannulation)
The principle advantage: TEE yields near perfect views in seconds.
Use of Resus-TEE in Cardiac Arrest
Currently there are a few uses of resus-TEE in cardiac arrest! These include identifying etiologies of cardiac arrest, Improving positioning of Compressions to improve CPR quality, Identifying certain rhythms not seen on surface electrodes to include Fine V. Fib.
Hand placement during CPR: Compression over LVOT or aortic root can have dramatically lower rates of ROSC!
Also Fine V-Fib can appear like Asystole! Resus TEE can help prevent this misinterpretation and changes your treatment algorithm dramatically!
Undifferentiated Shock: TEE allows for the identification and serial monitoring of different types of shock.
See our episode on undifferentiated shock for more.
Trauma: Resus-TEE helps ID areas of trauma and structural injury. Interestingly in one study of post-trauma care Resus-TEE identified Left Ventricle Outflow Tract (LVOT) Obstructions which benefit from beta-blocker therapy!
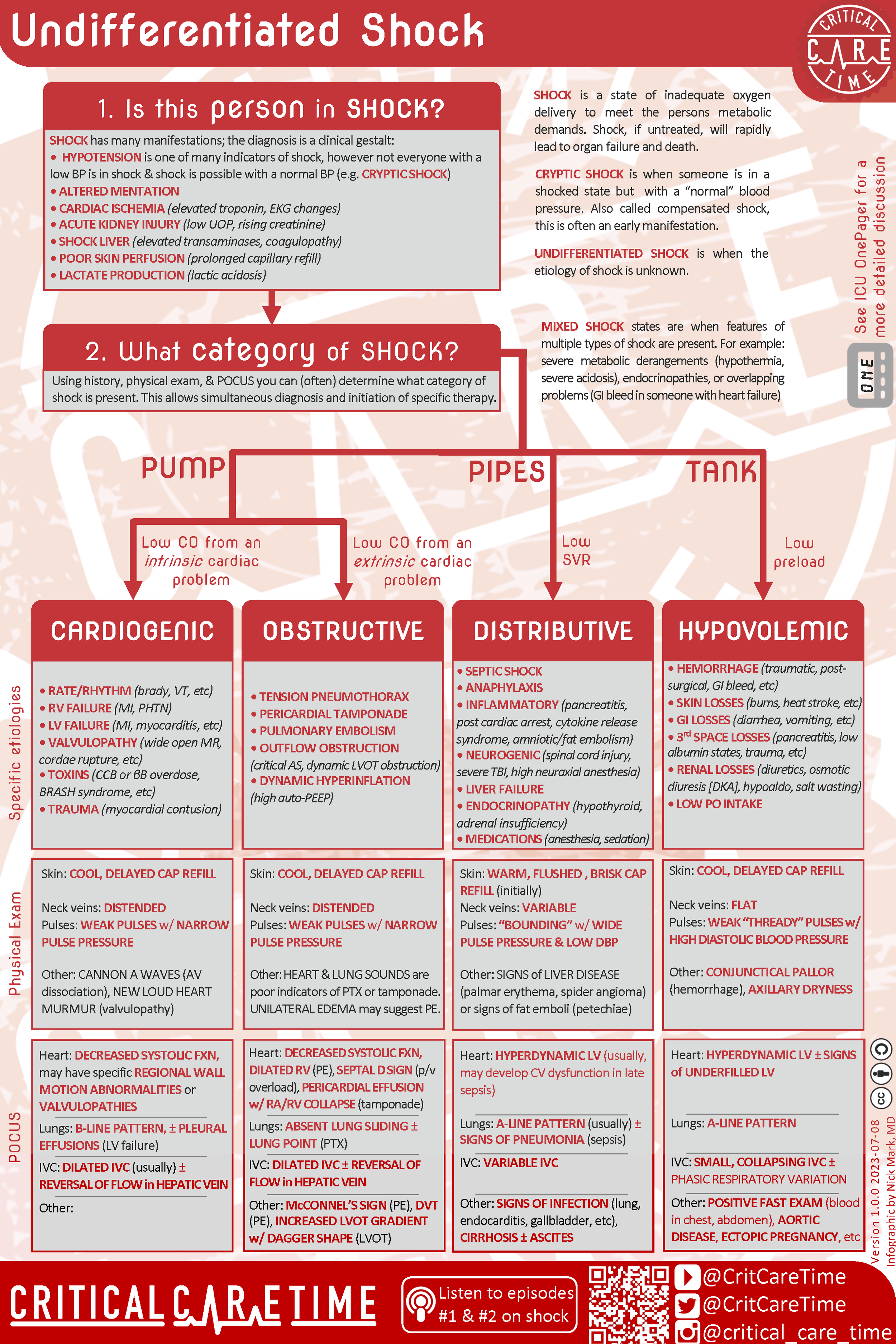
CCT Infographic on Undifferentiated Shock
What are the downsides with resus-TEE?
The risks associated with TEE are typically associated with sedation and airway management. In the Resus-TEE setting patients are already intubated so these complications are mitigated. In general this leaves complications from direct trauma of the ultrasound probe on surrounding tissues. Examples include minor oropharyngeal and GI bleeding.
Compared to the risks of more invasive procedures like PA catheter insertion, the risks of Resus-TEE are generally much lower and the procedure is well tolerated.
Logistical challenges of implementing Resus-TEE
Typically Resus-TEE probes are kept in the ICU and ER setting where they can be used to help ascertain etiology of shock in critical patients.
Providers can often perform the procedure independently after only a handful of supervised insertions.
Use of simulated patients allows for even faster acquisition of skills needed for successful Resus-TEE performance
In terms of training and certification there are no strict training or certification courses required to performed Resus-TEE.
Similar to traditional POCUS use, supervised use and review of acquired images is important.
There are whole day and half-day Resus-TEE courses available for additional training (see below)
There are disposable TEE probes available for use however these provide lower quality images and do not provide additional benefit for initial phenotyping of shock.
Where can I find more information on resus-TEE courses, registry and other resources?
www.resuscitativetee.com is a great resource that includes a patient registry for centers performing resus-TEE where data is being generated regrading how patient care is being improved by resus-TEE
BONUS: What is the current state of medicolegal liability around POCUS application?
Current data is limited though analysis of Canadian Medico-legal POCUS cases found 15 cases. Most of these were related to a failure to perform POCUS when indicated.
In some cases liability was related to misinterpretation or misapplication of POCUS.
BONUS: What else is Dr Ross Prager working on?
Ross is interested in finding innovative solutions to enhance researcher productivity and impact. To achieve this, he developed Resub, a tool that automatically formats manuscripts for submission to any journal in minutes. Resub saves researchers significant time and effort, addressing the global issue of over 23 million hours spent annually on manuscript formatting. You can try check out Resub.app now with a free demo.
Audio
Video
-
Teran F, Prats MI, Nelson BP, et al. Focused transesophageal echocardiography during cardiac arrest resuscitation: jacc review topic of the week. J Am Coll Cardiol. 2020;76(6):745-754.
Arntfield R, Lau V, Landry Y, Priestap F, Ball I. Impact of critical care transesophageal echocardiography in medical-surgical icu patients: characteristics and results from 274 consecutive examinations. J Intensive Care Med. 2020;35(9):896-902.
-
-
Undifferentiated Shock
Cardiac Arrest